January/February 2014
Alzheimer's Disease and
the Blood-Brain Barrier
By Norbert Myslinski, PhD
Today’s Geriatric Medicine
Vol. 7 No. 1 P. 26
The skull, cerebrospinal fluid, and blood-brain barrier (BBB) all protect the human brain and thus demonstrate its importance. Like a locked fence around your home, the BBB prevents intruders from entering. It also controls the movement of cells and molecules between the blood and the fluid that surrounds the nerve cells.
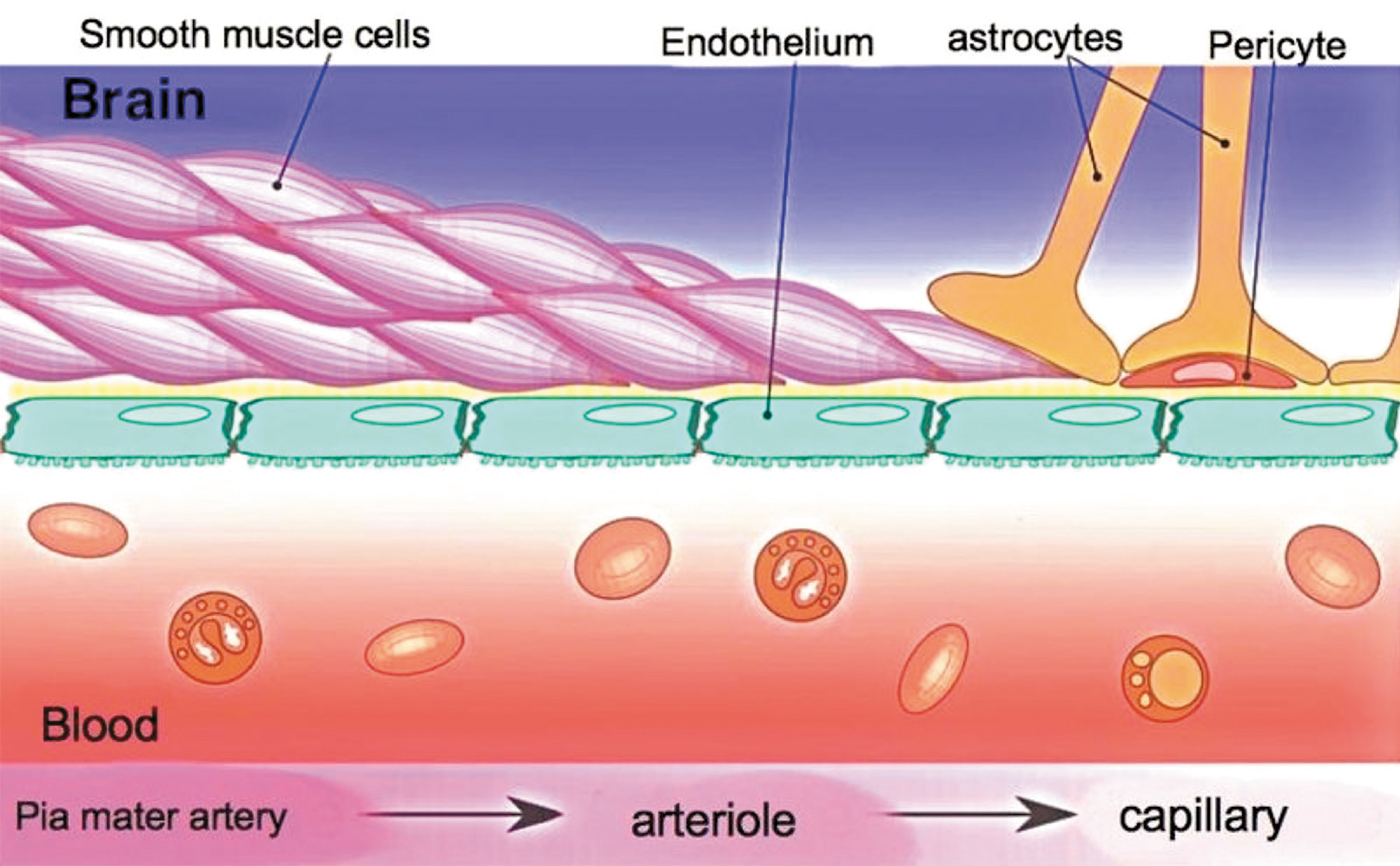
Nowhere else in the body is there such an anatomical barrier. It is made up of astrocytic feet around capillaries, a thicker basement membrane, and tight junctions between endothelial cells. Bacteria, toxins, drugs, and metabolic waste products, such as urea, find it difficult to cross.
Access is relative, however, and not absolute, since necessary substances such as oxygen and hormones can easily cross. Essential nutrients and glucose, the primary source of energy for the brain, cross with the help of certain transport proteins. Pericytes help regulate the barrier’s permeability (see Figure 1 below).
Pathology
The breakdown of the BBB may be involved in several brain diseases, such as multiple sclerosis, meningitis, epilepsy, and Alzheimer’s disease (AD). Although multiple sclerosis has long been thought of as a disease of the immune system, some consider it a disease of the BBB.
In multiple sclerosis, the immune system attacks myelin, a substance that insulates and protects neuronal axons. Normally, the white blood cells of the immune system cannot pass the BBB. However, during a multiple sclerosis attack, a section of the BBB breaks down in the brain or spinal cord, allowing T lymphocytes to cross over and attack the myelin.
Meningitis is the inflammation of the meninges, or membranes surrounding the brain and spinal cord, caused by bacteria, viruses, and other microorganisms. This inflammation, in turn, breaks down the BBB and allows neurotoxins to enter the brain. This may lead to common symptoms of meningitis such as headache, fever, and vomiting.
Research has shown that a BBB breakdown, caused by pathology or iatrogenic manipulations, can trigger acute or chronic seizures in epilepsy or other nonepileptic conditions.1 By measuring the BBB’s permeability to albumin and other tracers, BBB breakdown was found in rat and human brains with status epilepticus. Artificially disrupting the BBB with mannitol increased the number of seizures in rats.
Changes in the BBB also may aggravate or even cause AD by increasing the amounts of beta-amyloid and other toxins in the brain. This vascular dysfunction precedes the neuronal dysfunction and degeneration.
At the November 2013 convention of the Society for Neuroscience, Berislav V. Zlokovic, MD, PhD, professor and chair of the department of physiology and biophysics at the University of Southern California and the director of the Center for Neurodegeneration and Regeneration, discussed the BBB and neurodegeneration in such diseases as AD. Important substances involved in this relationship include the receptor for advanced glycation end products (RAGE) and apolipoprotein E (APOE).
RAGE transports beta-amyloid into the brain. Studies show that there are increased levels of RAGE in the blood vessels of a mouse model of AD. This increase is associated with an increased entry of beta-amyloid into the brain as well as raised levels of inflammatory chemicals, oxidative stress markers, and endothelin-1, a vasoconstrictor. Blocking the beta-amyloid/RAGE interaction reversed these effects. This supports the view that changes in RAGE in cerebral blood vessels contribute to the pathology of AD, and that it is a potential target for the development of new AD therapies.
Regarding APOE, humans carry two copies consisting of any combination of its three isoforms: APOE2, APOE3, and APOE4. Two APOE4 genes create the strongest genetic risk factor for AD; the combination increases the risk by 400% to 1,500% compared with APOE3/3 carriers. The 10 other genes most frequently associated with AD (eg, clusterin, phosphatidylinositol binding clathrin assembly protein) have only a 10% to 15% increased risk.
APOE4 homozygotes decrease the age of onset of AD by 15 years and have been associated with other neuropathologies, such as multiple sclerosis, stroke, frontotemporal dementia, and Parkinson’s disease, but to a much lower degree. APOE4 has several toxic effects on the cerebrovascular system that contribute to neurodegenerative changes.
One such effect is a beta-amyloid–independent effect mediated by cyclophilin A in brain vascular pericytes that leads to loss of cerebrovascular integrity and BBB breakdown resulting in neuronal injury. Imaging and biochemical studies indicate that AD patients have a greater breakdown of the BBB compared with neurologically healthy controls. Postmortem studies indicate that BBB degeneration is greater in AD patients who carry the APOE4 isoform. BBB breakdown in AD patients also is associated with decreased pericytes in the hippocampus.
The involvement of proinflammatory cyclophilin A in this effect was demonstrated by using humanized APOE transgenic mouse lines. These studies showed that APOE4, but not APOE2 and 3, leads to an age-dependent progressive BBB breakdown by activating a cyclophilin A pathway in brain capillary pericytes. The activation of this pathway leads to enzymatic degradation of BBB basement membranes and tight junctions, followed by neuronal uptake of multiple neurotoxins and reductions in microvascular blood flow. These vascular defects precede neuronal dysfunction and neurodegenerative changes.
APOE2 and 3, on the other hand, suppress the cyclophilin A pathway by means of lipoprotein receptor-related protein 1. They have a high affinity for lipoprotein receptor-related protein 1, whereas APOE4 has a low affinity. Cyclophilin A therefore can be considered a target for treating APOE4-mediated neurovascular injury and the resulting dysfunction.
Another effect of APOE4 is a beta-amyloid–dependent effect of decreasing the clearance of beta-amyloid from the brain into circulation, thus leading to its buildup in the brain. The beta-amyloid/APOE2 and 3 complexes are cleared at a substantially faster rate than the beta-amyloid/APOE4 complexes. The different APOE isoforms, therefore, regulate the clearance of beta-amyloid from the brain at different rates.
Therapy
The BBB also can be detrimental to the brain by preventing access to medicine, just as the locked gate around your home may keep out life-saving personnel the same way it keeps out intruders. Therefore, the BBB can prevent potentially therapeutic drugs from reaching the brains of AD patients. One reason many AD clinical trials have failed is because the drugs could not cross the BBB in significant amounts. Gaining access to the brain has long been an essential part of the development of drugs to treat brain disorders.
Whether using antibiotics to treat brain infections or dopamine to treat Parkinson’s disease, it has always been a challenge to find ways to deliver therapeutic drugs into the brain. Biochemists overcome the BBB by making the drugs smaller, more lipid soluble, and less ionized. They also piggyback drugs onto endogenous transport mechanisms, including receptor-mediated transporters for insulin or carrier-mediated transporters of glucose or amino acids. This is analogous to being escorted through the locked gates around our homes.
We also can tear down a part of the gate to obtain access to the home. In a similar manner, we can temporarily disrupt the BBB with high-intensity ultrasound or the use of vasoactive substances such as bradykinin. But one of the newest methods of improving access to the brain involves nanotechnology.
Liposomes containing nanoparticles can transport drugs across the BBB. Flurbiprofen is an FDA-approved drug that can lower beta-amyloid in the brain if it can gain entry. Professor Claus Pietrzik, of the Institute of Physiological Chemistry and Pathobiochemistry at Johannes Gutenberg University in Mainz, Germany, embedded flurbiprofen in nanoparticles to see whether it could help with crossing the BBB. He used an in vitro cell culture model of the BBB to measure the efficiency of crossing as well as the drug’s effectiveness after it crossed. The results showed efficient crossing and lowering of beta-amyloid levels.2
Nanoparticle delivery systems to the brain also have been intensely studied with antineoplastic drugs. For example, polyethylene glycol–coated hexadecylcyano-acrylate nanospheres have successfully accumulated in and suppressed rat gliosarcomas.
The better way to deliver AD drugs to the brain would be to find a way to safely open and close the BBB, which would be like finding a key to the locked fence around your home. Researchers at Cornell University believe they have found such a key: adenosine.3 When adenosine activates its receptors on cells in the BBB, it opens a gateway for large molecules to enter the brain. The researchers also found that Lexiscan, an adenosine-based drug approved by the FDA for other uses, can work on the adenosine receptors to open the BBB for about three hours. Although the data are from work on mouse brains, adenosine receptors are found on the same BBB cells in humans.
These studies showed that large molecules such as dextrans and antibodies could enter the brain. In a transgenic mouse model, they allowed beta-amyloid antibodies to enter the brain safely and bind to beta-amyloid plaques associated with AD. The advantages of this technique are that it can be turned on and off, the drug that is transferred does not lose any of its effectiveness as with some piggybacking techniques, and it does not create a problem by leaving nanoparticles in the brain.
Related work is progressing to help with multiple sclerosis. However, in this case, researchers are attempting to keep the BBB closed to prevent destructive immune cells from entering the brain.
Final Thoughts
In summary, the BBB is of critical importance in both the pathology and treatment of AD. Increased levels of RAGE in the BBB may lead to an increase of beta-amyloid in the brain. The increased risk of AD associated with APOE4 may be due to a BBB-related decrease in the clearance of beta-amyloid from the brain, and a cyclophilin A-related BBB breakdown leading to an influx of neurotoxins and neuronal degeneration. On the other hand, the BBB prevents therapeutic drugs from entering the brain. But many mechanisms of overcoming this barrier are becoming available, including the use of carrier proteins, nanoparticles, and adenosine receptors.
Researchers are changing the way they think about the BBB. Instead of being an enemy, it is now being thought of as an ally. Rather than its being simply a cause of AD and an impediment to providing therapeutic medicine, it is now thought of as a biological tool that can be finely manipulated to help treat and possibly cure AD.
— Norbert Myslinski, PhD, is a neuroscientist and faculty member in the dental and nursing schools of the University of Maryland in Baltimore and the director of the “Physiology of Aging” course. He founded the Baltimore Chapter of the Society for Neuroscience.
Click to enlarge image
— Image courtesy of Armin Kübelbeck and Creative Commons
References
1. Meister S, Zlatev I, Stab J, et al. Nanoparticulate flurbiprofen reduces amyloid-β42 generation in an in vitro blood-brain barrier model. Alzheimers Res Therap. 2013;5(6):51.
2. Marchi N, Angelov L, Masaryk T, et al. Seizure-promoting effect of blood-brain barrier disruption. Epilepsia. 2007;48(4):732-742.
3. Carman AJ, Mills JH, Krenz A, Kim DG, Bynoe MS. Adenosine receptor signaling modulates permeability of the blood-brain barrier. J Neurosci. 2011;31(37):13272-13280.
|