March/April 2016
Namaste Care Improves Quality of Life for Dementia Patients With the increasing life span of people in most countries and aging identified as the major risk factor for the development of it, dementia has become a major health care problem. With no effective prevention or treatment on the horizon, the number of people with an irreversible dementia is rapidly increasing. There are currently 5.2 million Americans with Alzheimer's disease and other dementias, a number projected to increase to 7.1 million in 2025 and to 13.8 million in 2050.1 Alzheimer's disease is the only disease among the top 10 causes of death in America that cannot be prevented or cured, and there is no medication that will significantly slow its progression. Therefore, there exists a great need for the development of strategies that will provide effective, affordable, and compassionate care for people with dementia, enabling them to live with quality in their lives, both physical and cognitive, throughout the progression of their disease. Dementia affects every aspect of an individual's life. Cognitive impairment causes a loss of independence and decreases quality of life. Factors that lead to a decreased quality of life include the following: • Communication difficulties prevent involvement in activities that depend on verbal communication between a person with dementia and a care partner, whether professional or family members. For an individual with dementia, misunderstanding a care partner's intention can lead to rejection of the care the partner is trying to provide.2 If a care partner insists on providing the care, the individual may shout or strike out in self defense. Such a situation is very stressful for both the person with dementia and his or her care partner and can transform a long term care setting or a home into a battlefield.3 These behaviors are often interpreted as aggressive and frequently lead to the administration of antipsychotics, which have several dangerous side effects.4 • Executive dysfunction leads to the inability to initiate meaningful activity by an individual with dementia. In earlier stages of the disease, activity professionals provide meaningful activities but often for only a few hours per day. Optimal quality of life requires continuous activity programming that includes both physical and mental exercises.5 However, cognitive impairment and communication difficulties make it impossible for a person with advanced dementia to participate in many of these activities. He or she may either sit on the periphery of an activity, often sleeping; sit in a corridor in a long term care setting; or remain isolated in his or her room.6 In such situations, individuals with dementia experience boredom that can cause physical or verbal agitation. Physical agitation can include restlessness, repetitive movements, and pacing, which increases the risk of falls. Verbal agitation can result in disruptive vocalization.7 • Psychiatric conditions that are unrecognized or untreated may lead to a significant decrease in quality of life in individuals with dementia. The most important of these is depression, which is very common in people with dementia and is often undiagnosed and undertreated.8 Depression is a risk factor for rejection of care, escalating into abusive behavior,9 and for agitation.10 Other conditions that can decrease quality of life are hallucinations, if they become disturbing to an individual with dementia, and apathy, an often unrecognized condition that can result in weight loss11 and failure to thrive. • Unrecognized or undertreated pain can also decrease the quality of life of people with dementia. Pain is very common in these individuals,12 who often cannot verbally report their pain, describe its location, or characterize its severity. Several programs attempting to improve the quality of life for people with dementia have been developed, each of which addresses one or more of these factors.13 However, some of these programs exclude people with advanced dementia14 and some require additional staff,15 which is not always realistic in the current fiscal environment of nursing home facilities. Therefore, there is a need for a comprehensive program for individuals with advanced dementia that is sustainable over time in the long term care setting without additional funding. Namaste Care, a program that fulfills these criteria, is described below. Namaste Care
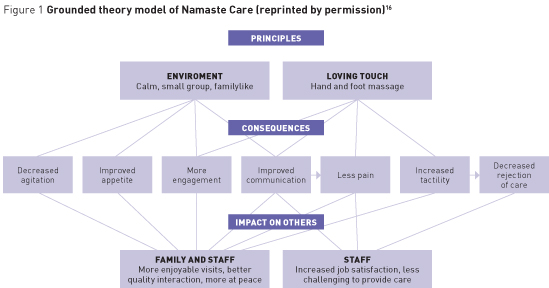
A comfortable environment includes space that is available for at least two hours in the morning and two hours in the afternoon for the Namaste Care program. Namaste Care involves a group activity, requiring space adequate to accommodate eight to 10 residents in reclining wheelchairs or lounge chairs. The optimal space is a room that can be secured so that supplies can be safely stored when not in use for the program. If a dedicated room is not available, other rooms can be adapted. Often the dining room is used. When the residents finish the meal, the room is cleaned and then made to look as homelike as possible. The room for Namaste Care should be free from distractions. With soft lighting, relaxing music, and the scent of lavender permeating the room, the environment calms even agitated residents. Participants in Namaste Care are placed in lounge chairs if they are not in reclining wheelchairs. They are carefully positioned and assessed for pain or discomfort. A blanket may be tucked around them to increase their sense of safety. Patients' participation in Namaste Care is welcomed by family members, who feel that their loved ones are at peace.16 Family visits become more satisfying because of improved communication and the opportunity to participate in some activities, such as hand massage. Namaste Care can be provided in a patient's room if he or she is unable to go to the Namaste Care room. The principles of Namaste Care are relevant even for the care of patients in a hospice setting or at home. Seasons Hospice and Palliative Care based in Rosemont, Illinois, and with sites nationwide, provides Namaste Care for all its patients with advanced dementia. Namaste Care principles can be useful in a hospital setting as well.17 Namaste Care does not require additional staffing. The number of residents in the room must be at least equal to the ratio of nursing assistants to residents. One staff person, usually a nursing assistant, is assigned to the program, scheduled to begin after most of the residents have completed their breakfast and to end before lunch. The afternoon session typically begins at 2 PM and continues until 4 PM. A Namaste carer is always present in the Namaste Care room; the residents are never left alone. Teamwork is vital in making the program succeed. Because a Namaste carer may not have all of his or her assigned residents in the program, other staff members watch his or her residents while he or she is caring for other staff members' residents. Occasionally activity professionals lead the program. Establishing Namaste Care does not require additional staff; however, it simply requires reassignment of residents for the program's duration. The person conducting the program might be either a nursing assistant who likes the program and provides it for the entire day or several staff members who rotate in the Namaste Care room. Loving touch is the second main principle of Namaste Care. In contrast to usual care that is task oriented and provided in a time-efficient manner, the care provided in the Namaste Care room is compassionate, slow, and person centered. Loving touch includes massage of hands and feet, applying to residents' faces a moisturizing cream with a scent reminiscent of the past, and carefully brushing residents' hair or providing a gentle scalp massage. This loving touch approach to care includes the Namaste carer talking to the resident, regardless of his or her ability to speak. Participation in Namaste Care addresses all of the factors listed above that decrease the quality of life. A comfortable environment and the presence of others decrease agitation18 because the residents are no longer isolated. The participants also experience reduced apathy, which promotes improved appetite and prevents weight loss.11 Namaste Care participants are offered beverages on a continuous basis to prevent dehydration, which can result in hospital admission.19 The continued presence of the Namaste carer and the chance to be with other residents provide the opportunity for engagement with others and the environment. The loving touch activities described above engage the resident as well. Increased engagement provided by the program director, volunteers, or other residents increases the communication ability of the participants. Both the Namaste carers and family members are often astonished when a resident who was completely mute starts talking to them.16 Improved communication makes family visits more enjoyable and families report that they visit more often. Enjoyment of touch in Namaste Care makes participants more receptive to touch by care partners, which is required in providing care for the activities of daily living, such as bathing, dressing, and toileting. Therefore, patients are less likely to reject care and become combative. This makes the work of care partners less challenging, and together with better communication between carers and program participants, increases their job satisfaction. Decreasing or eliminating rejection of care allows the discontinuation of neuroleptic medications that are often prescribed to treat this condition.20 For several reasons, pain control is improved in Namaste Care. First of all, all residents are carefully assessed for pain when they enter a Namaste Care room. Second, improved communication enables residents to report pain location and intensity. Third, pain is decreased by the loving touch and may be decreased without increasing administration of analgesics. Lastly, increased engagement decreases the concentration of residents on mild discomfort they may perceive as pain.16 Conclusion — Ladislav Volicer, MD, PhD, FAAN, FGSA, a professor at the University of South Florida School of Aging Studies in Tampa, also has academic appointments at the Charles University in Prague, Czech Republic, and the University of Western Sydney in Australia. References 2. Volicer L, Van der Steen JT, Frijters DH. Modifiable factors related to abusive behaviors in nursing home residents with dementia. J Am Med Dir Assoc. 2009;10(9):617-622. 3. Volicer L. Is your nursing home a battlefield? J Am Med Dir Assoc. 2012;13(3):195-196. 4. Rochon PA, Gruneir A, Gill SS, et al. Older men with dementia are at greater risk than women of serious events after initiating antipsychotic therapy. J Am Geriatr Soc. 2013;61(1):55-61. 5. Volicer L, Simard J, Pupa JH, Medrek R, Riordan ME. Effects of continuous activity programming on behavioral symptoms of dementia. J Am Med Dir Assoc. 2006;7(7):426-431. 6. Simard J. Silent and invisible; nursing home residents with advanced dementia. J Nutr Health Aging. 2007;11(6):484-488. 7. Sloane PD, Davidson S, Buckwalter K, et al. Management of the patient with disruptive vocalization. Gerontologist. 1997;37(5):675-682. 8. Volicer L, Frijters DH, Van der Steen JT. Underdiagnosis and undertreatment of depression in nursing home residents. Eur Geriatr Med. 2011;2(6):332-337. 9. Galindo-Garre F, Volicer L, Van der Steen JT. Factors related to rejection of care and behaviors directed towards others: a longitudinal study in nursing home residents with dementia. Dement Geriatr Cogn Dis Extra. 2015;5(1):123-134. 10. Volicer L, Frijters DH, Van der Steen JT. Relationship between symptoms of depression and agitation in nursing home residents with dementia. Int J Geriatr Psychiatry. 2012;27(7):749-754. 11. Volicer L, Frijters DH, Van der Steen JT. Apathy and weight loss in nursing home residents: longitudinal study. J Am Med Dir Assoc. 2013;14(6):417-420. 12. Van der Steen JT, Regnard C, Volicer L, Van Den Noortgate N, Sampson EL. Detecting pain or distress in people with dementia: an appraisal of two strategies. Eur J Palliat Care. 2015;22(3):110-113. 13. Morley JE, Philpot CD, Gill D, Berg-Weger M. Meaningful activities in the nursing home. J Am Med Dir Assoc. 2014;15(2):79-81. 14. Spector A, Thorgrimsen L, Woods B, et al. Efficacy of an evidence-based cognitive stimulation therapy programme for people with dementia: randomised controlled trial. Br J Psychiatry. 2003;183:248-254. 15. Graessel E, Stemmer R, Eichenseer B, et al. Non-pharmacological, multicomponent group therapy in patients with degenerative dementia: a 12-month randomized, controlled trial. BMC Med. 2011;9:129. 16. Manzar BA, Volicer L. Effects of Namaste Care: pilot study. Am J Alzheimers Dis. 2015;2(1):24-37. 17. St John K, Koffman J. Acceptability of Namaste Care for patients with advanced dementia being cared for in an acute hospital setting. End Life J. 2015;5(1):e000013. 18. Stacpoole M, Hockley J, Thompsell A, Simard J, Volicer L. The Namaste Care programme can reduce behavioural symptoms in care home residents with advanced dementia. Int J Geriatr Psychiatry. 2015;30(7):702-709. 19. Phelan EA, Borson S, Grothaus L, Balch S, Larson EB. Association of incident dementia with hospitalizations. JAMA. 2012;307(2):165-172. 20. Fullarton J, Volicer L. Reductions of antipsychotic and hypnotic medications in Namaste Care. J Am Med Dir Assoc. 2013;14(9):708-709. |