September/October 2016
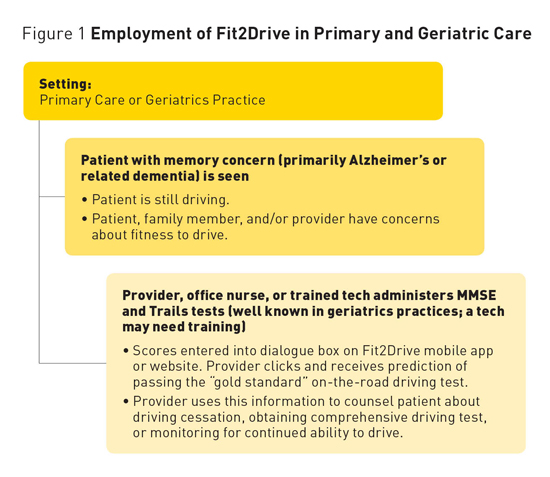
Fit2drive: New App Predicts On-Road Driving Ability in Patients With Dementia To assess driving fitness in patients with dementia, researchers have developed an app that predicts on-road driving skills using the results of two well-known cognitive tests. It is well known that Alzheimer's disease and related chronic progressive dementias place affected individuals at risk for unsafe driving but also eventually leave impaired individuals unable to drive. For the large number of adults who depend upon their personal automobiles for transportation, driving cessation has a profound impact on their functional independence, self-esteem, mood, social life, ability to participate in community activities, and ability to obtain everyday necessities and needed services.1 It is no surprise then that some patients and their families have described the driving issue as "the biggest problem we've ever had to face"2 and that physicians and other primary care providers are often called upon for advice related to driving cessation. While individuals with dementia are more likely than unimpaired older adults to be found to be unsafe drivers and to evidence more rapid decline in driving performance, there is considerable evidence that patients in the earliest stages of dementia may be able to continue driving for some time. For example, data from two longitudinal studies comparing drivers in the early stages of dementia with unimpaired drivers indicated that 88% of those with very mild impairment (having a Clinical Dementia Rating [CDR] scale score of 0.5) and 69% of those with mild impairment (a CDR score of 1) are able to pass a standardized road test. Follow-up testing found that adequate driving ability continued for a median two years for those with a CDR score of 0.5 and for one year for those with a CDR of 1.3-5 Driver Assessment According to the recent (third) edition of the Clinician's Guide to Assessing and Counseling Older Drivers (http://geriatricscareonline.org/ProductAbstract/clinician's-guide-to-assessing-and-counseling-older-drivers/B022),6 a driver evaluation plan begins with a screening phase in which a patient's physical and cognitive capabilities are reviewed. Noncognitive factors that may affect driving include chronic medical conditions, impaired ambulation, sleep disorders (leading to falling asleep at the wheel), acute illness or recent surgical procedures (affecting short-term fitness to drive), behavior disorders and substance abuse, neurological conditions, medications (causing drowsiness, dizziness, and confusion particularly), and visual acuity.7 The Clinical Assessment of Driving Related Skills found in the Clinician's Guide includes visual field deficits; visual acuity; rapid pace walk; strength and range of motion of the neck, shoulders, elbows, fingers, and ankles; ability to complete a maze test; Montreal Cognitive Assessment; Trail-Making Test Part B (longer than 180 seconds suggests referral for comprehensive evaluation); and the clock drawing test. Additionally, there is a set of self-evaluation questions (Have you ever gotten lost while driving? Had any accidents? Had others criticize your driving?) that are useful in interviewing patients8 contained in the Driving and Dementia Toolkit, also available online (www.rgpeo.com/media/30422/d%20%20d%20toolkit%20pt%20crgvr%20eng%20with%20 The second stage involves treatment of any medical conditions identified and a comprehensive driver evaluation, usually conducted by a driving specialist, including in-office and standardized on-road testing similar to the evaluation described in the next section. The outcome may be a finding that the patient is fit to drive with or without restriction, needs rehabilitation or recovery before returning to driving, or needs to stop driving.6 Development of Fit2Drive Tests Used A score below 19 was classified by the developers as impaired, a score between 19 and 23 was classified as borderline impairment, and a score between 23 and 30 was classified as normal.9 More recently, the Alzheimer's Association (2016) suggests that a score of 20 to 24 is indicative of mild dementia, 13 to 20 of moderate dementia, 12 and less of severe dementia.11 It has been generally thought that individuals who score less than 24 on an MMSE have an increased risk of having an automobile accident.12,13 However, if an individual scores in the borderline or impaired range, this does not mean they can be assumed to be entirely unfit to drive, as this measure was designed to determine cognitive impairment but not driving skills. Trail-Making Test, Part B In a study of more than 500 adults, the reported mean time to complete Trails B in control subjects was 81.5 compared with 136 for individuals with mild cognitive impairment and 140 for individuals with Alzheimer's disease.19 The average age in this group was 72.4, which was lower than in our sample. DORE The test takes place in a dual-brake vehicle provided for participants. It is scored on several components, including risks of a collision/accident rating, driver rating, and the driving course difficulty level. There is no penalty for the errors or bad driving habits that are typical of unimpaired drivers. Upon completion, the scores are coded, and a coding sheet is transmitted to DriveABLE. Results are based on a proprietary computer algorithm21 and presented as a score within the range of normal safe driving, which is scored as a pass; a score within the upper range of normal-competent driving, which receives a borderline pass; or a score outside the range of normal-competent driving, which is considered a fail. Study Sample Analysis Based upon the relative predictive strength of the various in-office test scores, the MMSE and Trails B time in seconds were selected for our Fit2Drive Calculator. Since there were two predictors in this model, a second logistic regression analysis was run with these predictors to determine the overall predictive weight of both the MMSE and the Trails B. These weights became the basis of the prediction equation. The binary pass-fail outcome allows the predictive model to assess the sensitivity (ie, a true positive) and specificity (ie, a true negative) of the predictive outcomes compared with the on-road test. From these results, a contingency table can be created from the four possible outcomes (true positive, false positive, true negative, and false negative). The overall combination of the sensitivity and specificity is then graphed (called a receiver operating characteristic curve, which plots true positives against true negatives on the tests of interest) and the area under the curve provides an estimate of the overall accuracy of our predictors. For this analysis, the overall accuracy was 75%. If we printed a table with every possible combination of the MMSE score and Trails B time, the table would be 176 pages long and very clumsy to use during a patient consultation. To provide quick access to these predictions, we developed a calculator, Fit2Drive, based on an equation derived from our data. When a patient's MMSE and Trails B time scores are entered, the calculator provides the probability the patient will pass an on-road driving evaluation. Integrating Fit2Drive Into the Screening Stage of Driver Evaluation
The Fit2Drive calculator utilizes the total score from the original MMSE9 and Trails B time in seconds (Trails A should be administered first to provide the same amount of practice that the patients in the research study had prior to completing Trails B). A technician may be trained to administer these tests, but an untrained person may not obtain comparable results. The two scores are entered online or into the mobile app to obtain a prediction of the likelihood that the patient would pass the on-road driving test. Using the Fit2Drive Calculator Limitations Summary — Ruth M. Tappen, EdD, RN, FAAN, is a professor and eminent scholar in the Christine E. Lynn College of Nursing at Florida Atlantic University (FAU) in Boca Raton. She was the founder of the Memory and Wellness Center at FAU and has conducted a number of funded studies on Alzheimer's disease and related dementias. — Jamie Zahava Ramos, BA, is a graduate student in the department of psychology at FAU. — David O. Newman, PhD, is a biostatistician at the College of Nursing at FAU. He developed the predictor equation discussed in this article. — Matt Newman, BA, is president and CEO of SolveIT Consulting, Inc, which created the Fit2Drive website. References 2. Liddle J, Tan A, Liang P, et al. "The biggest problem we've ever had to face": how families manage driving cessation with people with dementia. Int Psychogeriatr. 2016;28(1):109-122. 3. Duchek JM, Carr DB, Hunt L, et al. Longitudinal driving performance in early‐stage dementia of the Alzheimer type. J Am Geriatr Soc. 2003;51(10):1342-1347. 4. Ott B, Heindel WC, Papandonatos GD, et al. A longitudinal study of drivers with Alzheimer disease. Neurology. 2008;70(14):1171-1178. 5. Ott BR, Daiello LA. How does dementia affect driving in older patients? Aging Health. 2010;6(1):77-85. 6. American Geriatrics Society. Clinician's Guide to Assessing and Counseling Older Drivers. 3rd ed. Washington, DC: National Highway Traffic Safety Administration; 2016. 7. Odell M. Assessing fitness to drive: part 2. Aust Fam Physician. 2005;34(6):475-477. 8. Byszewski A, Aminzadeh F, Robinson K, Molnar F, Dalziel W. The Driving and Dementia Toolkit for Patients and Caregivers. http://www.rgpeo.com/media/30422/d%20%20d%20toolkit%20pt%20 9. Folstein MF, Folstein SE, McHugh PR. "Mini-mental state." A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res. 1975;12(3):189-198. 10. Cockrell JR, Folstein MF. Mini-Mental State Examination. In: Copeland JRM, Abou-Saleh MT, Blazer DG, eds. Principles and Practice of Geriatric Psychiatry. 2nd ed. Chichester, West Sussex, England: Wiley; 2002:137-147. 11. Tests for Alzheimer's disease and dementia. Alzheimer's Association website. http://www.alz.org/alzheimers_disease_steps_to_diagnosis.asp. Accessed July 7, 2016. 12. Hogan DB. Which older patients are competent to drive? Approaches to office-based assessment. Can Fam Physician. 2005;51:362-368. 13. Lin MS, Skolnik, NS. Evaluation and Management of driving risk in dementia. Family Practice News. 2011;41:21. 14. Arbuthnott K, Frank J. Trail Making Test, Part B as a measure of executive control: validation using a set-switching paradigm. J Clin Exp Neuropsychol. 2000;22(4):518-528. 15. Dobbs BM, Shergill SS. How effective is the Trail Making Test (Parts A and B) in identifying cognitively impaired drivers? Age Ageing. 2013;42(5):577-581. 16. Lezak MD. Executive functions and motor performance. In: Neuropsychological Assessment. 3rd ed. New York, NY: Oxford University Press; 1995:650-685. 17. Reitan R. The relation of the trail making test to organic brain damage. J Consult Psychol. 1955;19(5):393-394. 18. Tombaugh TN. Trail Making Test A and B: normative data stratified by age and education. Arch Clin Neuropsychol. 2004;19(2):203-214. 19. Ashendorf L, Jefferson AL, O'Connor MK, Chaisson C, Green RC, Stern RA. Trail Making Test errors in normal aging, mild cognitive impairment, and dementia. Arch Clin Neuropsychol. 2008;23(2):129-137. 20. DriveABLE On-Road Evaluation. DriveABLE website. http://www.driveable.com/index.php/products/dore. Accessed July 7, 2016. 21. Dobbs AR. Accuracy of the DriveABLE cognitive assessment to determine cognitive fitness to drive. Can Fam Physician. 2013;59:e156-E161. |