September/October 2017
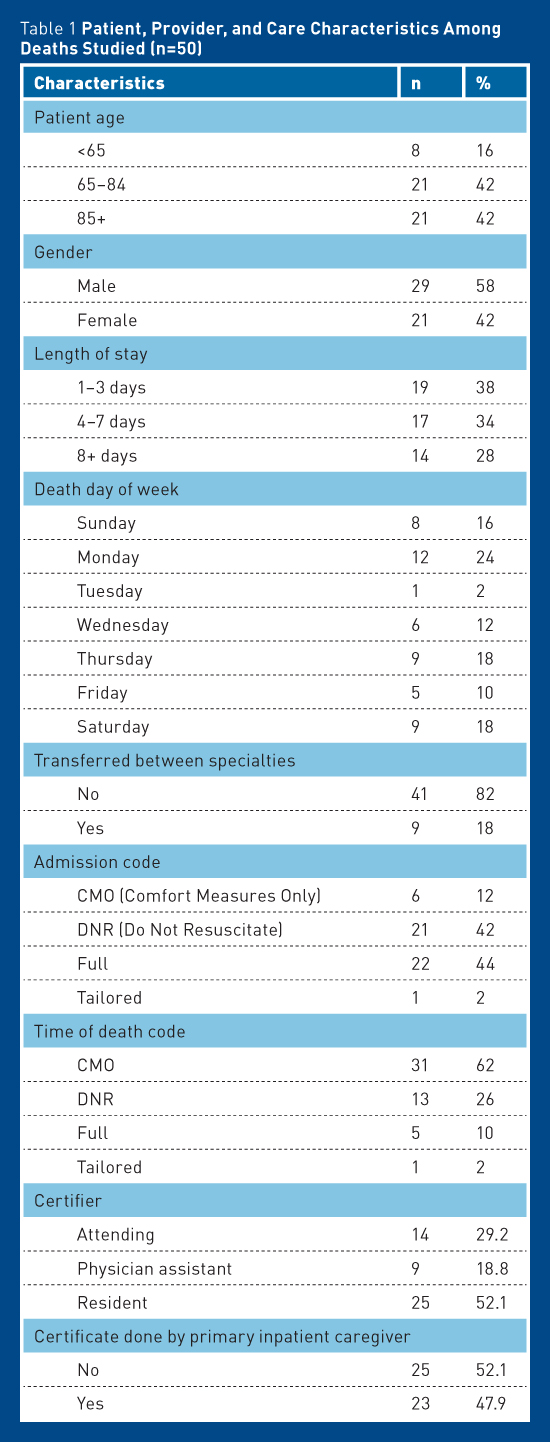
Research Review: Death Certificate Accuracy — Why It Matters and How to Achieve It Death certificate inaccuracy is a well-recognized problem at both the national and international levels. Infractions range from major, such as errors in identifying cause and manner of death, to minor, such as illegibility and incompleteness.1 Despite such known shortcomings, we continue to use these data at a state, national, and international level to inform research projects, direct funding streams, and determine health care goals. Multiple studies have looked at the underlying "why" of these inaccuracies, and the majority indicate a deficit in the training of the medical professionals asked to tackle this paperwork on a regular basis.1-8 Additional studies have then determined best options for addressing these deficits and have suggested targeted interventions for improvement.1-4,7-9 Since the majority of deaths in the United States occur in adults over the age 65, practitioners who care for geriatric patients play a key role in ensuring that submitted data reflect mortality in the United States as accurately as possible.10 It should therefore be a priority of current practice for providers to be educated in the tenets of death certificate completion. Defining the Problem: At Home and Abroad In the United States it is estimated that the rate of major errors (eg, incorrect cause of death [CoD], incorrect manner of death) found on death certificates completed at academic institutions is approximately 33% to 40%.1 Internationally, this rate at some hospitals rises as high as 80%,7,14-16 where factors such as infrastructure, need for translation between documentation and submission, and overall funding for diagnostics may play more significant roles.14,15 In the United States, the bulk of inaccuracies correlate to lack of training coupled with lack of understanding of the importance of this documentation.4-6,17 Primary Research The cache of 50 adult deaths assigned between May 2014 and October 2015 to one resident reviewer involved in this study provided the source cases for data collection. Each case underwent thorough chart review, and specific data were extracted. Data collected from the chart focused on patient and provider characteristics that were hypothesized to impact accuracy, such as patient length of stay, provider level of training, provider familiarity with patient, code status, etc (see Table 1). The number of underlying illnesses and complexity of medical presentation were recorded for reviewer information but not formally analyzed due to variations in medical record maintenance. Data collected from the death certificates were limited to CoD, contributory diagnoses, and manner of death. Researchers did not analyze duration of each contributing problem, tobacco use, or patient pregnancy status.
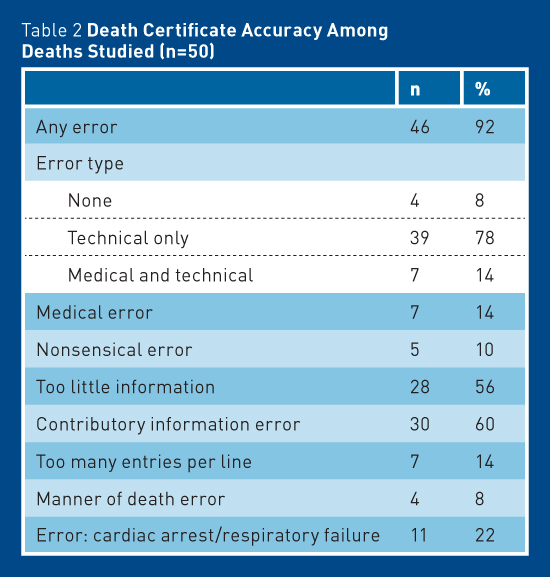
In the course of data collection and chart reviews, the accuracy reviewers underwent additional training in death certificate completion via online and literature-based self-teaching as well as off-site training with local medical examiners. Following training, reviewers established their own cause-of-death statements for each case. The original cause-of-death statement as well as the alternate were then analyzed and assessed for accuracy. Of note, the majority of original certificate errors were evident from a technical standpoint without requiring a full medical record review. Completely accurate certificates as well as points of inaccuracy were then identified and tabulated. Results: In Brief
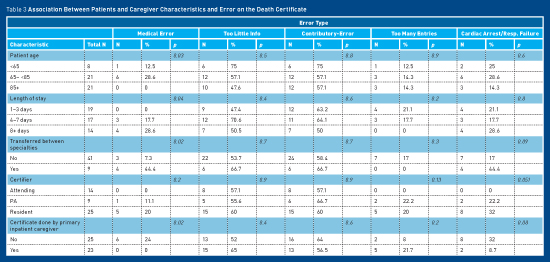
Given the high error rate overall, there were very few trends identified (see Table 3). No patient characteristics were significantly associated with level of accuracy. Level of medical training—thought to be a likely association with accuracy—was also not statistically significant overall. However, level of training was significant when it came to "medical" errors. No attending-level providers were assigned "medical" errors on their certificates. In addition, cardiac or respiratory arrest were incorrectly entered as immediate CoD on 11 of 50 certificates, none of which was completed by attending-level providers.
While no patient characteristics were predictive of error rate, it is notable that 84% of our adult medicine population deaths occurred in patients older than 65, evenly divided between those aged 65 to 84 and those aged 85 or older. Discussion Multiple studies have explored possible interventions in this arena. Suggestions include hour-long didactic sessions, day-long interactive seminars/workshops, independent paper or online instruction review, training videos, and retrospective feedback on audited certificates. The majority of these studies demonstrate higher yield from interactive formats, ie, seminars and workshops.1-4,7-9 A small study from Vermont in 2005 suggested an intervention that seems uniquely beneficial to the teaching hospital setting. These researchers recommended a two-part process including the following:1 • Provide an annual hour-long didactic session to refresh learners at all levels on the basic tenets of death certification and expose those who have never undergone training to proper methods for accuracy and clarity. • Elevate the completion of the death certificate to a team-based learning opportunity by encouraging teams to complete them together. The certificate thereby has greater potential for accuracy, and the team has the best opportunity for processing, reflection, and retention. For practitioners who lack access to formalized didactics and/or who do not interact in team-based teaching services, online modules and written instructions may be the most accessible options. In this spirit, included below are the guidelines to inform the reader's death certificate completion process going forward. The authors also recommend further online self-education as offered by the Centers for Disease Control and Prevention,18,19 as well as Brooks' and Reed's 2015 article "Principles and Pitfalls: A Guide to Death Certification."11 Components i. Chronic obstructive pulmonary disease exacerbation;* • Manner of Death: Natural, accident, homicide, suicide, undetermined. Most providers will complete death certificates for natural deaths only. Medical examiners should be called for all others, including deaths related to hip fracture, as they tend to qualify as accidents, and deaths related to a history of malicious injury, as those may be homicide. • Timeline: Located to the side of the CoD statements. It clarifies duration of disease presence to time of death and may be used to inform research questions pertaining to patterns of disease progression. • Contributing Factors (ie, comorbidities or other significant conditions): This portion can have multiple entries and should include any significant diagnoses that do not directly contribute to the CoD narrative. Clues and Clarifications • CoD should include only one entry per line and not all lines need be used depending on available information (see above). • "Cardiac arrest," "respiratory arrest," and "old age" are not acceptable entries under causes of death. *avoid abbreviations The authors acknowledge that the above guidelines are not exhaustive, and the challenges faced in completing death certificates accurately will continue to be fraught with best medical estimates as opposed to decisive facts. As a result, we can rarely be 100% confident as to what caused a death and, therefore, must accept that our data cannot be 100% accurate. What they can be, however, are thoughtful, informed, and collaborative. The majority of providers who care for geriatric patients will be called upon to complete death certificates. However, few among us will take the time to consider where the data go and why they matter. By glossing over this process, we are missing the opportunity to learn from our patients in death as we did in their lives, to improve the medical care and familial support that we provide as individuals and as institutions, and to impact the direction of health care on the national scale. — Emily Carter, MD, is a recent graduate of the Baylor College of Medicine Geriatrics Fellowship. She is a board-certified family physician and will return to Maine Medical Center as an attending physician this fall. — Christina Holt, MD, MSc, is research director for family medicine and director of the Preventive Medicine Residency Program at Maine Medical Center. Prior to returning to academics, she was a medical examiner in a practice in rural Maine and has done research using both birth and death certificate data for comprehensive community care. — Amy Haskins, PhD, is the research navigator for the Maine Medical Center Department of Family Medicine. Her background in epidemiology and research design helps all members of the department design and complete research, quality improvement, and evaluation projects. References 2. Aung E, Rao C, Walker S. Teaching cause-of-death certification: lessons from international experience. Postgrad Med J. 2010;86(1013):143-152. 3. Azim A, Singh P, Bhatia P, et al. Impact of an educational intervention on errors in death certification: an observational study from the intensive care unit of a tertiary care teaching hospital. J Anaesthesiol Clin Pharmacol. 2014;30(1):78-81. 4. Ong P, Gambatese M, Begier E, Zimmerman R, Soto A, Madsen A. Effect of cause-of-death training on agreement between hospital discharge diagnoses and cause of death reported, inpatient hospital deaths, New York City, 2008-2010. Prev Chronic Dis. 2015;12:140299. 5. Wexelman BA, Eden E, Rose KM. Survey of New York City resident physicians on cause-of-death reporting, 2010. Prev Chronic Dis. 2013;10:E76. 6. Williams L, Dewey H, Kapp MB. Long-term complication: Florida's death certification process and long-term care. Int J Risk Saf Med. 2011;23(3):139-147. 7. Maharjan L, Shah A, Shrestha KB, Shrestha G. Errors in cause-of-death statement on death certificates in intensive care unit of Kathmandu, Nepal. BMC Health Serv Res. 2015;15:507. 8. Myers KA, Farquhar DR. Improving the accuracy of death certification. CMAJ. 1998;158(10):1317-1323. 9. Smith Sehdev AE, Hutchins GM. Problems with proper completion and accuracy of the cause-of-death statement. Arch Intern Med. 2001;161(2):277-284. 10. Kochanek KD, Murphy SL, Xu JQ, Tejada-Vera B; Centers for Disease Control and Prevention, National Center for Health Statistics. Deaths: final data for 2014. https://www.cdc.gov/nchs/data/nvsr/nvsr65/nvsr65_04.pdf. Updated April 3, 2017. 11. Brooks EG, Reed KD. Principles and pitfalls: a guide to death certification. Clin Med Res. 2015;13(2):74-82. 12. Thornton RG. Death certificates. Proc (Bayl Univ Med Cent). 2006;19(3):285-286. 13. Mortality data. Centers for Disease Control and Prevention, National Center for Health Statistics website. https://www.cdc.gov/nchs/nvss/deaths.htm. Updated August 8, 2017. 14. Binsaeed AA, Al-Saadi MM, Aljerian KA, et al. Assessment of the accuracy of death certification at two referral hospitals. J Family Community Med. 2008;15(1):43-50. 15. Hernández B, Ramírez-Villalobos D, Romero M, Gómez S, Atkinson C, Lozano R. Assessing quality of medical death certification: concordance between gold standard diagnosis and underlying cause of death in selected Mexican hospitals. Popul Health Metr. 2011;9:38. 16. Nielsen GP, Björnsson J, Jonasson JG. The accuracy of death certificates. Implications for health statistics. Virchows Arch A Pathol Anat Histopathol. 1991;419(2):143-146. 17. Degani AT, Patel RM, Smith BE, Grimsley E. The effect of student training on accuracy of completion of death certificates. Med Educ Online. 2009;14:17. 18. Centers for Disease Control and Prevention, National Center for Health Statistics. Physician's handbook on medical certification of death. https://www.cdc.gov/nchs/data/misc/hb_cod.pdf. Published April 2003. 19. Centers for Disease Control and Prevention, National Center for Health Statistics. Instructions for completing the cause-of-death section of the death certificate. https://www.cdc.gov/nchs/data/dvs/blue_form.pdf. Published August 2004. |